Technical Guide to Measuring
This guide aims to provide a protocol for the correct measurement and configuration of Aria Wheels ultra-lightweight wheelchairs. It integrates clinical and biomechanical assessment principles with the technical specifications detailed in the Aria wheelchair order forms.
An ultra-lightweight wheelchair is a complex orthosis: accurate measurement ensures propulsion efficiency, postural stability, and the prevention of pressure sores.
Preliminary Evaluation Guidelines
Before proceeding with parameter measurement, it is essential to observe the following guidelines:
Positioning: All measurements must be taken with the user seated on a flat, rigid surface, simulating the desired final posture.
Aria recommends: You can use one of our adjustable "demo" wheelchairs with a rigid carbon fiber seat to take measurements directly on an Aria model and obtain a dimensional comparison.
Tools: Exclusively use a rigid tape measure or a caliper. Using flexible measuring tapes that follow the body's curves generates errors by overestimating the true anatomical measurements.
Manufacturing Tolerance: Aria Wheels frames are manufactured with a tolerance of ± 5 mm.
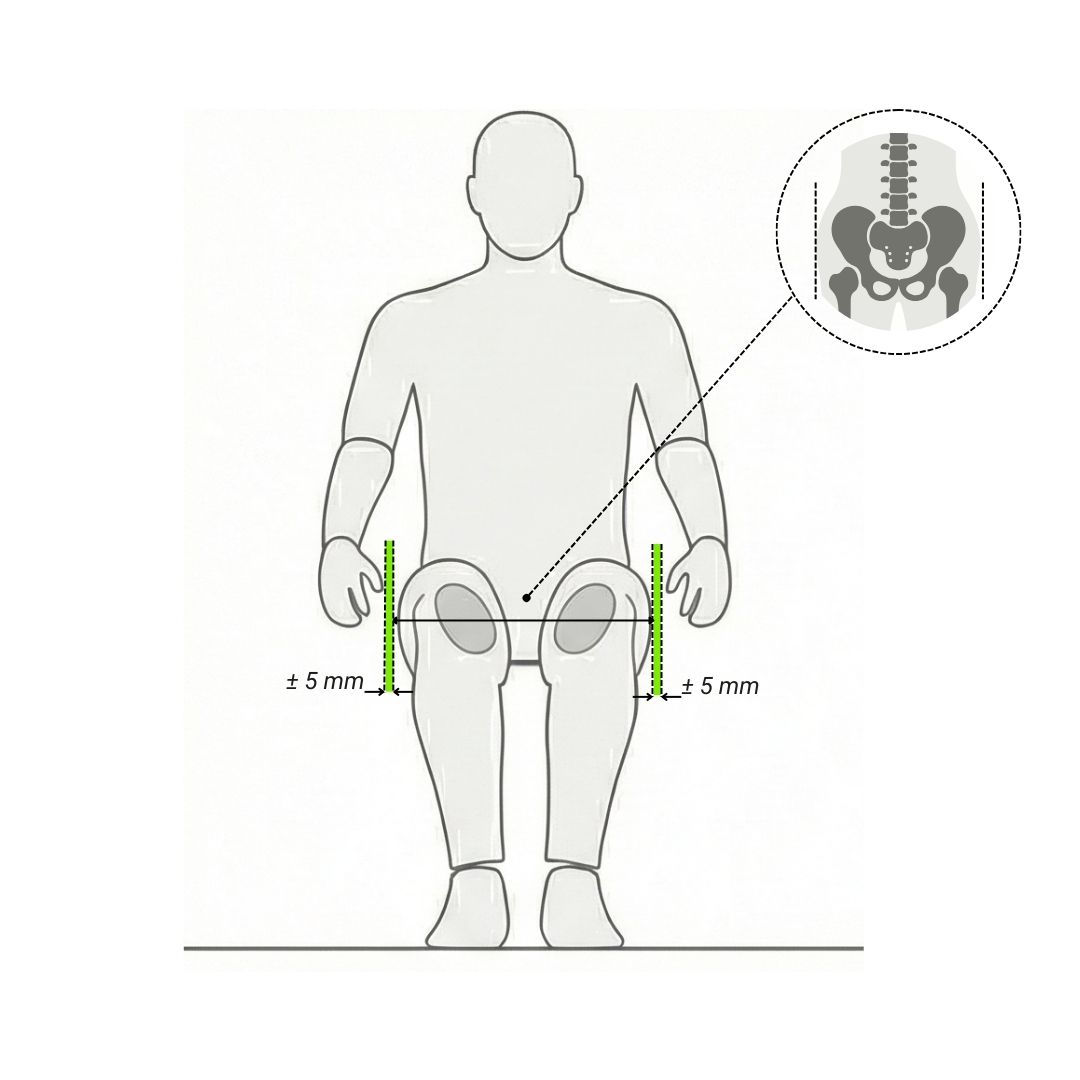
1. Seat Width (SW)
Aria Technical Definition:
The Seat Width (SW) measurement is considered by calculating the distance from the outer edge of one frame tube to the outer edge of the opposite tube.
How to take the anthropometric measurement on the user:
With the user seated, measure the bitrochanteric width (the linear distance between the two greater trochanters). It is crucially important to also measure the "bitrochanteric + excess" width, including any redundant adipose tissue in the hip area and considering the bulk of usual clothing (e.g., winter coats). Use rigid guides to prevent the tape measure from bending around the hips.
Clinical Indications:
The idea that a wider wheelchair guarantees greater comfort is a common misconception. An excessively wide seat prevents proper propulsion, compromises postural support, and induces the user to adopt lateral deviations (scoliosis) to seek stability.
Aria recommends: leave a tolerance space of ± 5 mm between the user's pelvis and the side guards.
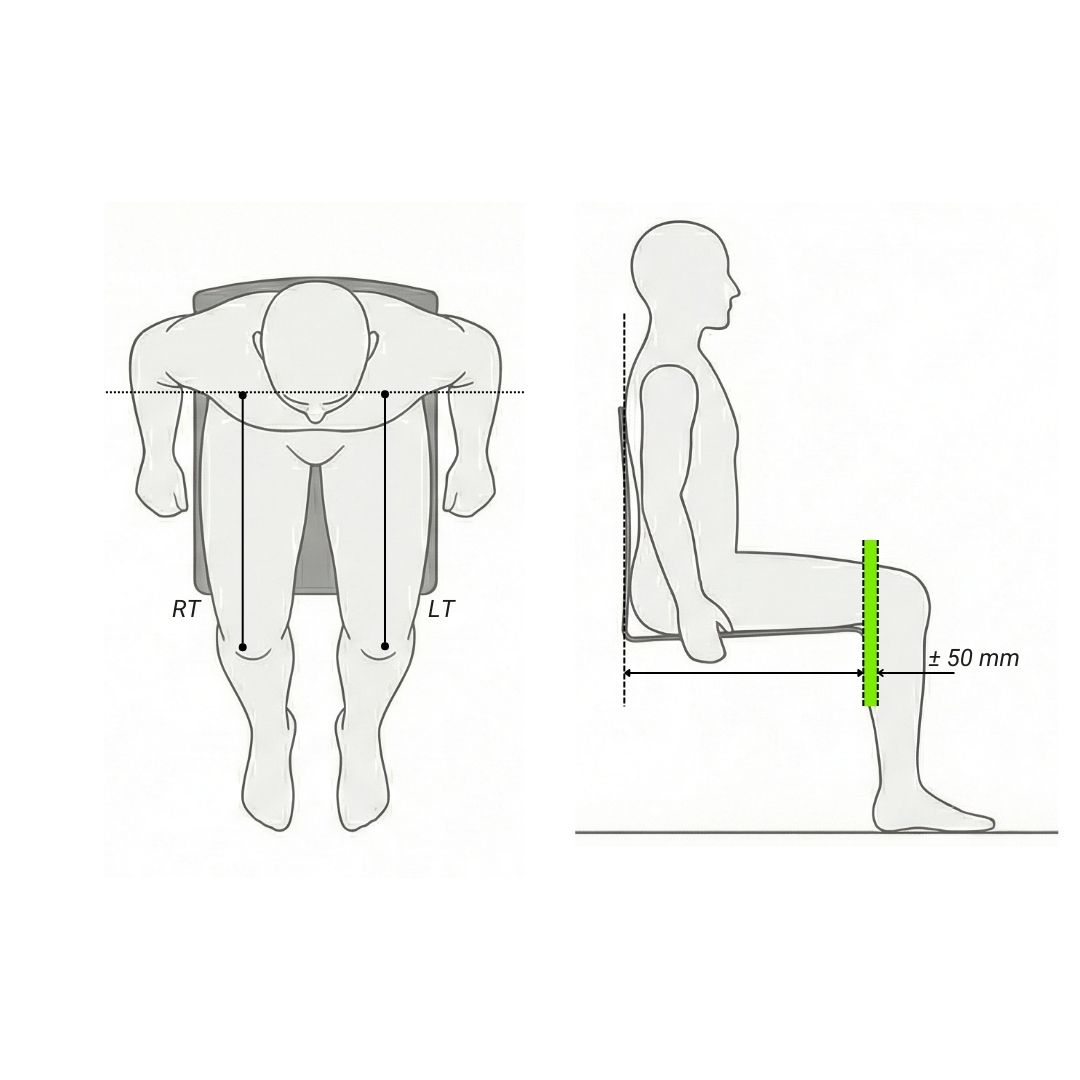
2. Seat Depth (SD)
Aria Technical Definition:
The Seat Depth (SD) measures the dimension from the front edge of the seat (upholstery or carbon fiber) to the backrest tube (or to the postural backrest for the Aria 1.0 model).
How to take the anthropometric measurement on the user:
Measure the distance from the sacral plane (or the ideal backrest line), along the axis of the femur, to the popliteal fossa (the back of the knee).
Pay attention to asymmetries: at this stage, it is vital to separately measure the right limb (Sacrum to Right Popliteal Fossa) and the left limb (Sacrum to Left Popliteal Fossa). In the presence of asymmetry (e.g., a difference in femur length or a structured pelvic rotation/obliquity), the shortest measurement must always be taken into consideration to establish the correct seat depth.
Clinical Indications:
Using the shortest measurement as a reference in case of asymmetry prevents the front edge of the seat from pressing against the popliteal fossa of the shorter leg, an event that would cause vascular problems and inevitably push the pelvis to slide forward into a posterior pelvic tilt (sacral sitting), negating lumbar support. If the seat is too short for both limbs, the support surface for the femurs is reduced, concentrating pressure peaks solely on the ischial tuberosities.
Aria recommends: maintain a free space of ± 50 mm between the popliteal fossa and the rigid edge (or upholstery) of the seat. If a rigid postural backrest is mounted, it is suggested to increase the frame's SD measurement by at least 2 cm to compensate for the bulk of the shell and hardware.
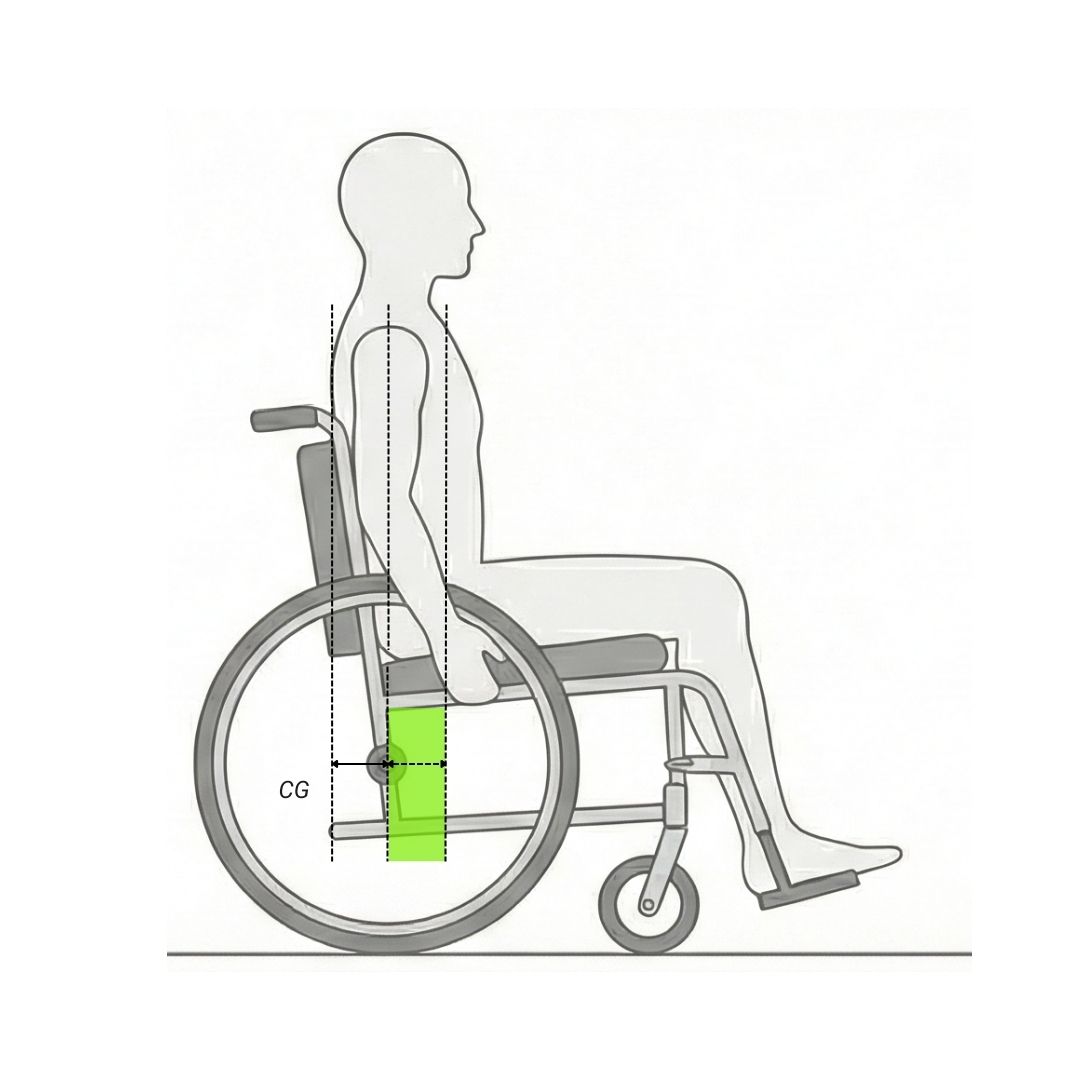
3. Center of Gravity (CG)
How to determine the CG:
The Center of Gravity is not an anatomical measurement, but a purely functional and clinical assessment. It depends on the user's experience, pathology, trunk control, and the presence of amputations or hypertonia.
Aria Technical Definition:
The Center of Gravity (CG) determines the balance point of the wheelchair and is calculated by measuring the distance from the axis of the backrest tube to the rear wheel axle (for the 1.0 model, the measurement is taken from the postural backrest foam to the wheel axle).
Aria recommends: if a postural backrest is mounted, the bulk of the shell and the actual position of the patient's back must be considered; consequently, the effective CG will be lower than the one selected on the frame. Therefore, as specified earlier regarding the need to increase the Seat Depth (SD), it is recommended to simultaneously consider a proportional increase in the CG parameter during configuration to maintain the desired setup unaltered.
Choosing the CG based on clinical and functional picture: The choice of CG determines how much of the user's mass rests on the rear wheels (traction) compared to the front wheels (rolling resistance).
Rearward CG (conservative setups, lower numerical values, e.g., 80-100 mm): By positioning the wheel axle further back, the wheelchair's wheelbase increases, and rearward tipping becomes extremely difficult.
Indicated for: users with bilateral lower limb amputations (where the loss of mass in the lower limbs shifts the body's center of gravity unnaturally towards the back); users with severe extensor spasms (which could suddenly push the torso backward) ; first-time users (newly spinal cord injured patients) who have not yet acquired mastery in wheelies and balancing.
Forward CG (active setups, higher numerical values, e.g., 110-150 mm): By moving the wheel axle forward, the chair is more responsive. The user has the wheels exactly under the shoulder joint, maximizing propulsion ergonomics and lightening the load on the front casters.
Indicated for: active users with good mastery of the device, and stable pathologies (e.g., polio sequelae, paraplegic spinal cord injuries) where overcoming urban obstacles by lifting the front wheels is a daily necessity.
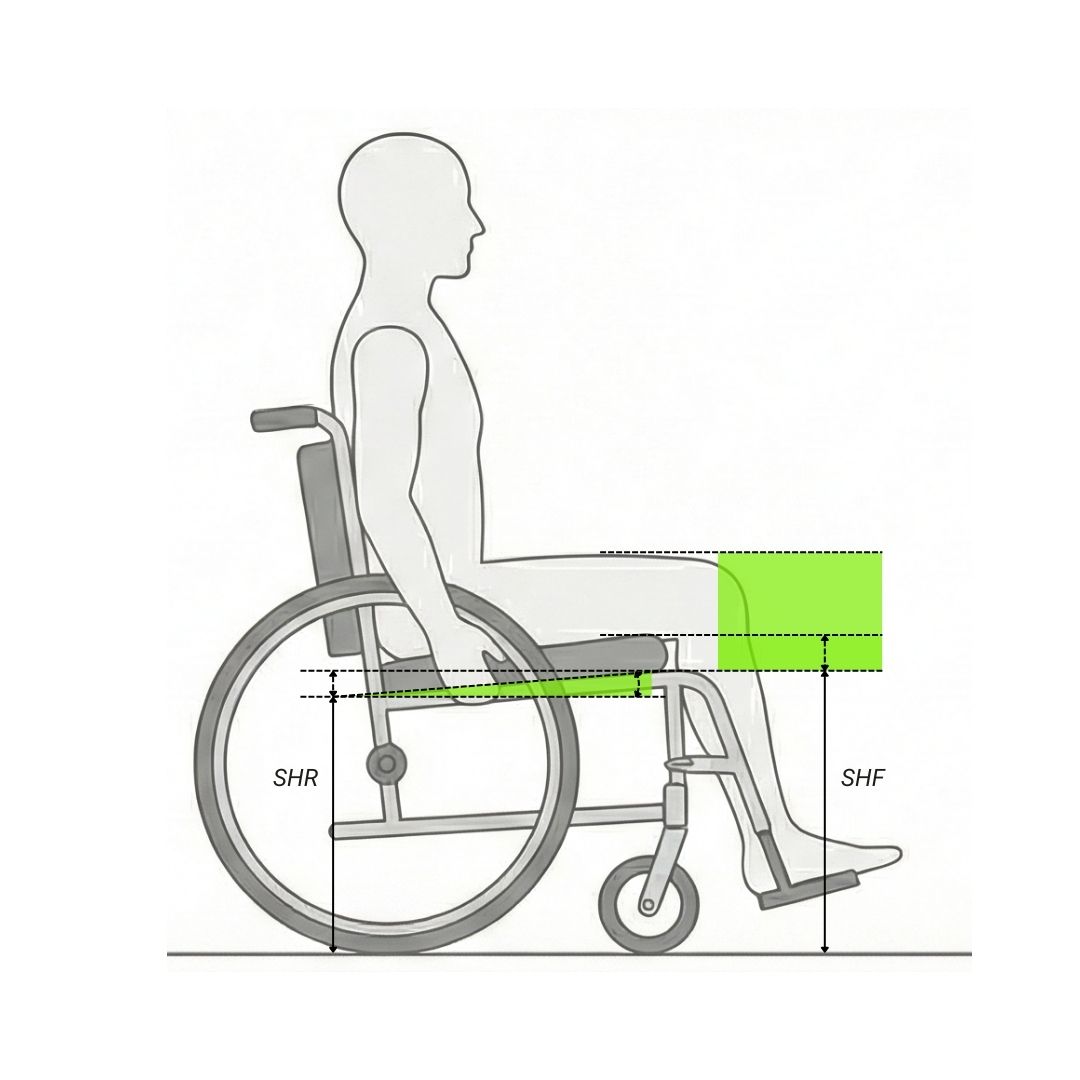
4. Seat Height: Front (SHF) and Rear (SHR)
Aria Technical Definition:
The front height (SHF) is measured from the ground to the front edge of the seat plane. The rear height (SHR) is measured from the ground to the rear edge of the seat plane (intersection with the backrest). In rigid frame models with a tiltable carbon fiber seat (CARBTS system, as on 2.0, Speciale, and Ultra), the heights can be adjusted by modifying the inclination (tilt) of the plane relative to the frame tubes, whose distance from the ground remains fixed. For models like Agile and Plixa, the setup is modified by acting on the position of the rear wheel axle and the height of the front fork.
How to detect environmental and functional parameters:
The seat height is determined by the length of the user's leg (to ensure a footrest height of about 25-50 mm from the ground to overcome small obstacles), but it must interface with the environment: bed height for transfers, car seat height, and accessibility under tables and desks.
Clinical and biomechanical indications:
Front Height (SHF): Determines accessibility to the surrounding environment (e.g., fitting under tables) and the ease of transfers. An excessive front height makes independent transfers complex and prevents the feet from touching the ground if necessary. A height that is too low exposes the footrests to the risk of hitting the ground or obstacles, and can increase pressure on the buttocks.
Rear Height (SHR) and Seat Angle (Dump): The difference between SHF and SHR creates the seat plane angle. A greater seat inclination (front part higher than the rear) increases pelvic stability, locks the femoral head in the acetabulum, and prevents the pelvis from sliding forward (retroversion). Conversely, a lower inclination (difference between SHR and SHF of 2 to 4 cm) leads to a "flatter" seat, therefore suitable for users who do not need to stabilize the pelvis and/or are capable of walking.
Pathological Considerations: Users with reduced trunk control greatly benefit from a more accentuated "dump" (seat inclination), which uses gravity to stabilize the torso against the backrest. However, an angle that is too extreme closes the hip angle and can generate ischial pressure peaks, which are not recommended for users at very high risk of pressure sores.
TECHNICAL NOTE: Integration of the Postural/Anti-decubitus Cushion
The technical diagrams and nominal dimensions provided in the Aria Wheels order forms do not consider the dimensions and bulk of any postural or anti-decubitus cushions. The choice of cushion (whether foam, air, fluid, or hybrid) is an integral part of the orthosis and actively modifies the anthropometry of the device. A cushion with a high-profile or anti-slip wedge ("anti-thrust") will raise the user's center of gravity, altering the effective Front and Rear Height (SHF/SHR) and modifying the relative position of the elbows and shoulders with respect to the wheels and backrests. Therefore, frame measurements must always be calibrated by calculating in advance the height and behavior (immersion/envelopment) of the chosen cushion during the assessment phase.
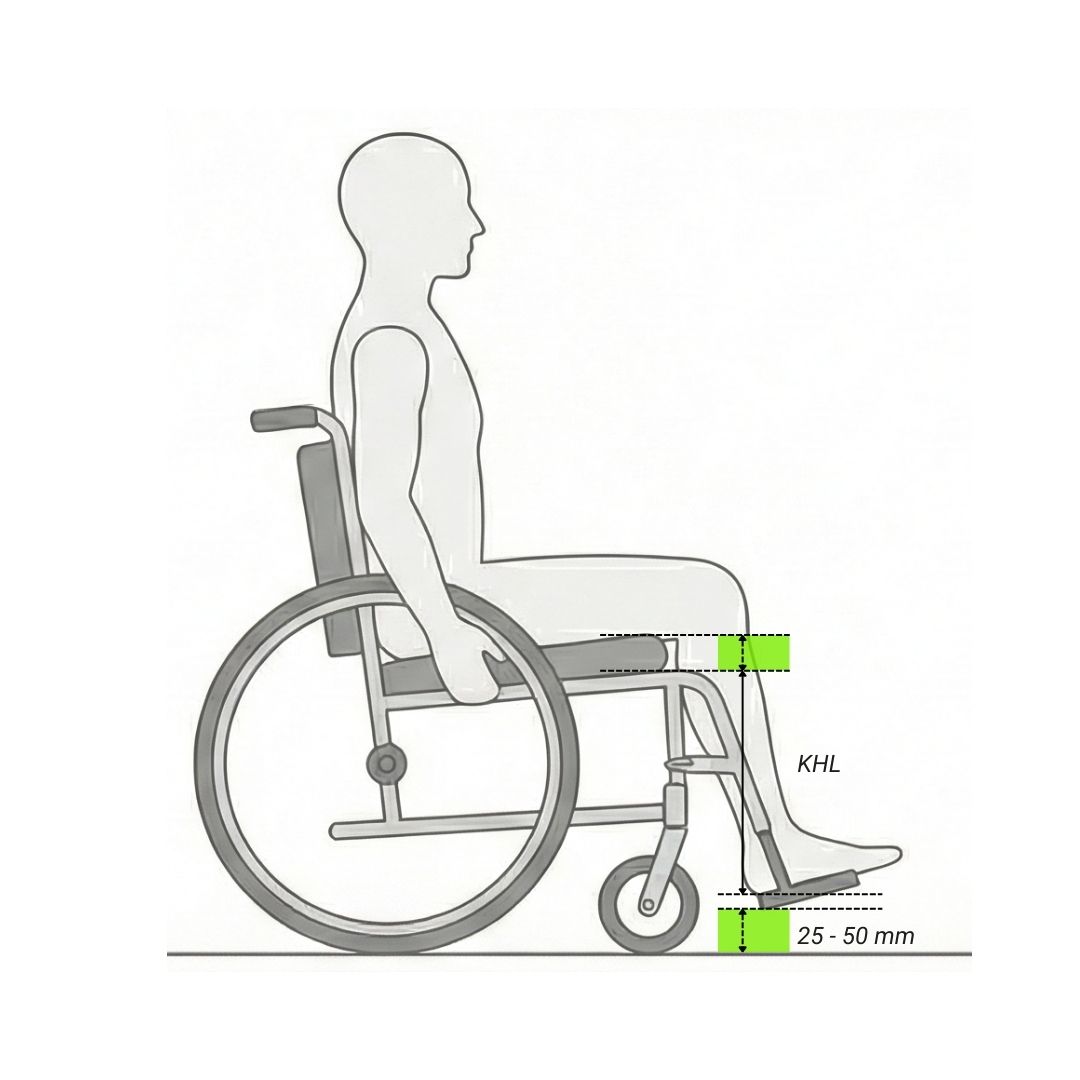
5. Knee to Heel Length (KHL)
Aria Technical Definition:
The KHL measurement refers to the distance between the front part of the seat and the footplate. Since this distance is influenced by the thickness of the cushion (which raises the user's knees), it is necessary to subtract the effective thickness of the cushion (considering its degree of sinking) from the anatomical measurement taken.
How to take the anthropometric measurement on the user:
With the knees and ankles at 90° (or at the flexion angle tolerated/desired by the user), measure from the popliteal fossa down to the base of the heel (Right and Left Popliteal fossa-heel). Also in this case, it is necessary to measure the right and left sides separately to identify any asymmetries in tibia length. Ensure the user is wearing their everyday footwear.
Clinical Implications:
If the KHL measurement set on the wheelchair is less than the user's actual leg length, it will induce excessive knee flexion, lifting the thighs off the seat and directing all compressive force exclusively onto the ischial areas. If the footplate is too far, the thighs will be stretched, the user will slide forward and use their feet for forced support, favoring pelvic deviations in the long term.
Safety warning: regardless of the user's leg length, the footrests should always be approximately 25-50 mm from the ground. This minimum distance is essential to allow adequate ground clearance, preventing the footrests from hitting the ground, getting stuck in stones or pavement cracks, or hindering transfers, while simultaneously ensuring correct support. In case of strong asymmetry between the right and left limbs, padding options on the single footplate should be evaluated to respect this rule.
Aria recommends: although this measurement is often adjustable, it is suggested to always consider the cushion thickness, as this will influence the position of the footrest relative to the seat.
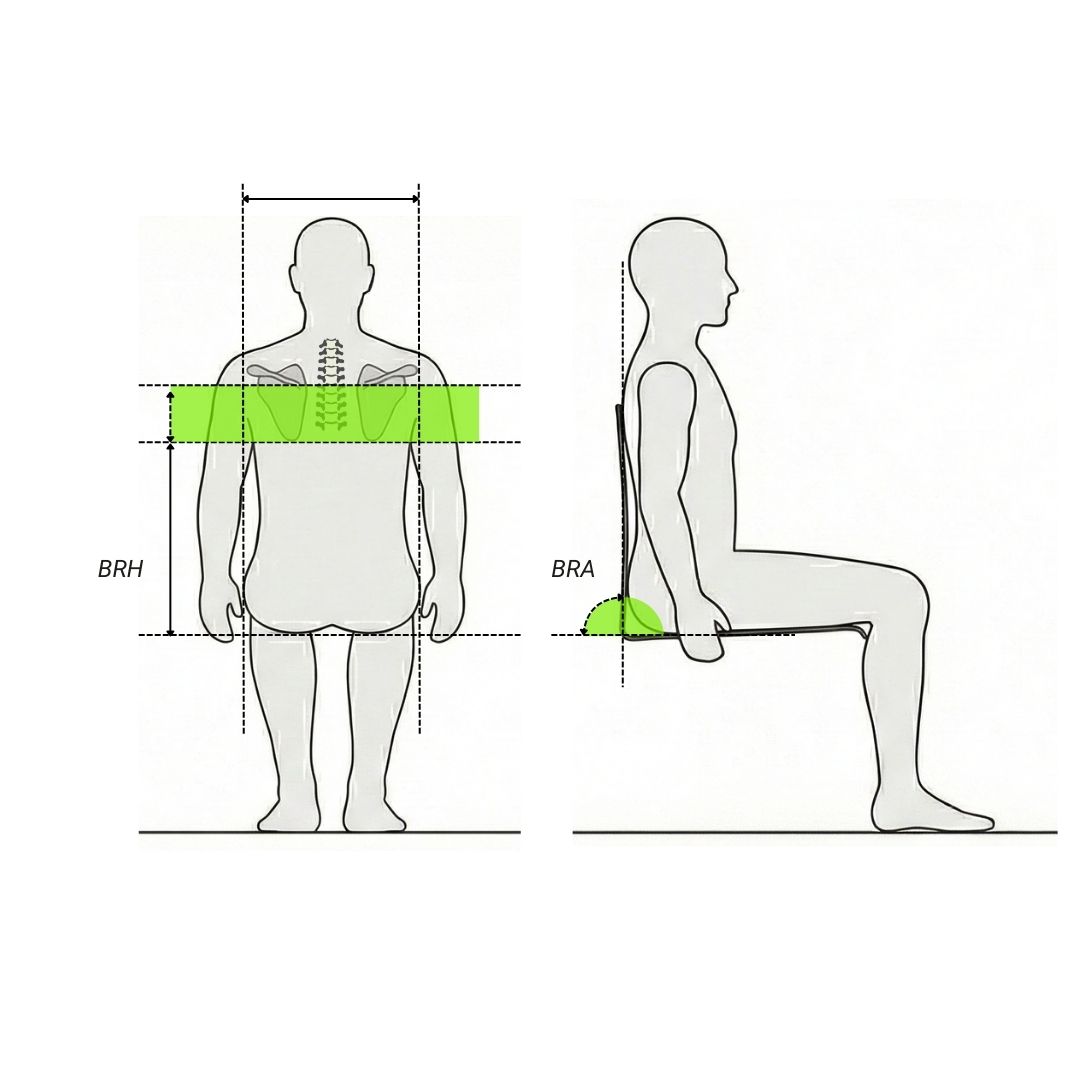
6. Backrest Height (BRH) and Angle (BRA)
Aria Technical Definition:
The BRH (Backrest Height) value is measured from the seat plane to the upper end of the backrest tube.
The BRA (Backrest Angle) value defines the angle of inclination of the backrest support tubes and/or the axis of the postural backrest shell measured relative to the ground.
How to take the anthropometric measurement on the user:
From the flat seating surface (at the level of the sacrum), measure the height along the spine up to the inferior angle of the scapula (Scapula-Sacrum measurement) for active users, or up to the prominent C7 vertebra (C7-Sacrum measurement) for users requiring extended trunk support. At this stage, it is also useful to record the trunk width for potential configuration of lateral supports or postural backrests.
Choosing the height based on the clinical picture:
Evaluating the backrest height requires a delicate balance between the need for support and freedom of movement.
Users with good trunk control (e.g., low spinal cord injury, paraplegia, early-stage spina bifida): it is advisable to opt for a lower backrest. The backrest should never exceed or interfere with the inferior angle of the scapula. A backrest that is too high in these users will limit shoulder extension, forcing them into inefficient propulsion biomechanics and predisposing them to rotator cuff pathologies.
Users with poor or no trunk control (e.g., high spinal cord injury, tetraplegia, advanced muscular dystrophies, severe multiple sclerosis): in cases of severe axial hypotonia or need for containment due to spinal asymmetries (kyphoscoliosis), providing greater support is mandatory. The backrest height must be taller to stabilize the thoracic vertebrae or, in some cases, it must integrate lateral support systems and headrests. The goal here is to maximize contact to manage pressure peaks and stabilize posture at the expense of freedom of movement.
Backrest Angle (BRA): the angle between the seat and the backrest (BRA) has a profound impact on seating biomechanics.
Closed angle (BRA > 90°): increases pelvic stability by limiting hip extension and locking the pelvis.
Open angle (BRA < 90°): A more reclined backrest angle is useful to accommodate users with hip flexion contractures or Range of Motion (ROM) limitations. However, it is vital to warn that excessive recline inevitably transfers pressure peaks and shear forces from the ischial area directly onto the sacrum.
Please note: in Aria Wheels order forms, the BRA (Backrest Angle) parameter indicates the inclination of the backrest tube measured relative to the vertical axis perpendicular to the ground ("external" measurement), and not the internal angle between seat and backrest.
Consequently:
BRA > 90° (e.g., 93°): the backrest is inclined forward towards the user (more "closed" internal angle)
BRA < 90° (e.g., 87°): the backrest is reclined backward (more "open" internal angle)
TECHNICAL NOTE: Postural Backrest Systems (Rigid)
Using a rigid postural system (e.g., carbon fiber or aluminum shells) is often the definitive leap in quality for positioning. These backrests offer greater support, better ergonomics respecting physiological curves (e.g., lumbar lordosis), and better correction of asymmetries (e.g., flexible scolioses).
It is crucial to remember that the installation of a rigid backrest and its mounting hardware will slightly reduce the effective Seat Depth (SD) available to the user; this must be carefully calculated during the measurement taking phase to prevent the seat from turning out too short.
7. Criteria for selecting the model based on the clinical picture
The prescription of an ultra-lightweight wheelchair must be based on the evaluation of residual functional potential, pathology stability, and the user's lifestyle. Below are the clinical recommendations for Aria Wheels models:
Aria 2.0, Agile, and Ultra for maximum adjustability: These rigid frame models are distinguished by a high degree of post-sale adjustability.
User profile: ideal for first-time users (e.g., recent spinal cord injuries), users with progressive or degenerative conditions (e.g., multiple sclerosis, spinal muscular atrophy) whose postural and biomechanical needs may change over time.
Clinical benefits: they allow clinicians and technicians to "fine-tune" the setup (center of gravity, heights) as the user gains competence in using the wheelchair or in response to changes in muscle trophism.

Aria 1.0 and Speciale: pure performance: Models 1.0 and Speciale represent the pinnacle in terms of lightness (transport weight ± 4 kg), structural rigidity, and propulsion efficiency. These models have minimal to no adjustments, acting as custom-welded/fixed frame wheelchairs.
User profile: active, expert users with a stabilized neuromotor and orthopedic clinical picture (e.g., traumatic paraplegia or polio sequelae stabilized for years).
Clinical benefits: the absence of moving parts eliminates kinetic energy dispersion during the push. However, an incorrect prescription during the order phase cannot be corrected later: it requires precise and final measurements.

Aria Plixa: the practicality of a folding frame: The Plixa is our only model equipped with a folding cross-brace frame.
User profile: users with stabilized pathologies who maintain a dynamic lifestyle and frequently need to stow the aid in small vehicles, or who have caregivers (e.g., elderly) for whom lifting a rigid frame is less manageable.
Clinical benefits: combines the need for reduced dimensions (width when folded of 350-370 mm).

Aria KID: adaptability and performance for the little ones: Aria KID is our rigid frame wheelchair model specifically designed for pediatric anthropometric proportions (SW starting from 240 mm).
User profile: children suffering from Infantile Cerebral Palsy (ICP), spina bifida, or developmental neuromuscular pathologies.
Clinical benefits: providing an extremely lightweight wheelchair (transport weight of ± 4.5 kg) prevents functional overload damage to delicate pediatric joints. The structure allows it to accommodate the child's growth while preserving spinal alignment and favoring independent exploration of the environment. Adequate backrest support (with customizable heights starting from 240 mm) is vital to prevent the formation of scoliosis or axial deviations during the bone growth phase.
Conclusion
The structural excellence and performance of Aria Wheels models are influenced by a strict correct geometric prescription. It is also fundamental to carry out an accurate measurement, conducted by trained technical personnel, in order to prevent secondary complications, improving the user's integration with the aid and ensuring correct biomechanical alignment during all daily activities.
Should you wish to delve into some technical details, or are interested in organizing a training course at your facility, we invite you to contact us.